
Coronavirus Crisis 2020: Crucial Covid Findings pt. I
The Coronavirus crisis of 2020 has pushed humanity to a point it has never been before, and while we’ve now transitioned into 2021, it doesn’t look like we’re nearing the end of this dark tunnel just yet. In fact, the exact same measures that seemed ineffective last year, are being applied again worldwide. In many countries, to an even stricter degree than before.
Over the past year, we’ve seen governments respond in like manner to what was reportedly an incredibly dangerous, deadly, and infectious virus that was taking the world by storm. The virus reportedly had people collapsing and dying in the streets in China, where the virus is said to have originated. This Guardian article from January 31st 2020 shows what they called “the chilling reality of the coronavirus outbreak.”

Before I get into the points I want to make in this article, I want to make a few things completely clear. I have no background in medicine, virology or any other relatable topic. Nor am I a doctor, a scientist, or anything of the kind. What I am, however, is concerned, very concerned, about the direction the world is heading in an extraordinarily fast pace. Just over one year ago things were still, what most would consider to be normal, everywhere. What exactly has happened over the past thirteen months, and how did we get to the point we now find ourselves?
To get a bit of an overview of this, I’ve written a document titled ‘Coronavirus Crisis 2020,’ which you can find on michaelgleesonmedia.com. In this document I’ve included a detailed timeline of relevant events that took place before, and during the coronavirus crisis. In doing so, I came across a lot of information that seems to directly contradict a lot of what governments and the corporate media all over the world have been proclaiming over the past couple months. A lot of which was derived directly from their very own sources, like for example the World Health Organisation (WHO), and The Centers for Disease Control and Prevention (CDC). Mainly pertaining to the level of danger and deadliness of the disease Covid-19, and the likelihood of asymptomatic transmission of the novel strain of coronavirus, SARS-CoV-2.
Most of the measures taken to combat this new virus; like lockdowns and business closures, have turned out to be nothing but different ingredients in an absolute recipe for disaster. We’re going to be looking at some of these measures and reading from different studies relating to these specific measures to see what effects they have had so far.
The topics that will be covered in this article are:
– Using the RT-PCR Method as a Diagnostic Tool for Covid-19
– Harm, Loss, and Damage Caused by Lockdowns, and Additional Deaths
– Surveillance Expansion and Government Overreach
– Asymptomatic Transmission
One more important point I would like to emphasise before starting, is to please not believe anything you read here. All sources can be found throughout this article, and all information discussed can be found in the Coronavirus Crisis document I mentioned earlier. Please take the time to look into these studies and events for yourself. That is really the main thing I’m trying to achieve with writing this article; to get people to inform themselves, rather than just believing the things they see and hear on the news, social media or elsewhere. And of course that also includes everything you read in this article.
Using the RT-PCR Method as a Diagnostic Tool for Covid-19
One thing that has been similar in every single country combatting the novel strain of coronavirus, is the primary method being used to detect and diagnose someone as infected with the novel coronavirus. This method is known as Reverse Transcription Polymerase Chain Reaction, or RT-PCR.
First, let’s look at what regular PCR is, without reverse transcription. Scitable, a platform started by the international scientific journal Nature, defines PCR as “a laboratory technique used to make multiple copies of a segment of DNA. PCR is very precise and can be used to amplify, or copy, a specific DNA target from a mixture of DNA molecules.” Merriam-Webster defines PCR as “an in vitro (meaning outside of the body) technique for rapidly synthesizing large quantities of a given DNA segment that involves separating the DNA into its two complementary strands, using DNA polymerase to synthesize two-stranded DNA from each single strand, and repeating the process.” Simply put, it is a technique used to amplify, or multiply a tiny sample of DNA millions of times in order to produce sufficient material to allow for genetic and molecular analysis.
What makes RT-PCR different from PCR is that RT-PCR uses RNA as a template instead of DNA, and RNA is what most viruses have as their genetic material. As the name suggests, the main difference is the additional step of Reverse Transcribing the RNA into what is called Complementary DNA, or cDNA. After that step the standard PCR procedure is used to multiply the cDNA making millions or even billions of copies, depending on the cycle threshold used. The amount of thermal cycles applied determine the amount of amplification, and thus the amount of genetic material you end up with.
I’m not going to delve too deeply into the exact workings of the PCR method, as there are many other sources to find about this online from people more qualified to talk about it than I am.
One of those people is Kary Mullis, the inventor of the PCR method for which he won the Nobel Prize in Chemistry in 1993. The following clip is taken from a conference held in Santa Monica, California in 1997, titled Corporate Greed & AIDS. The clip shows Mullis being asked about the misuse of PCR regarding the detection of the HIV virus. He goes on to explain that ‘misuse’ isn’t the right word, but rather that its results are often misinterpreted. “With PCR, if you do it well, you can find almost anything in anybody. […] It allows you to take a very miniscule amount of anything and make it measurable, and then talk about it at meetings like it’s important. […] It’s just a process that’s used to make a whole lot of something out of something. It doesn’t tell you that you’re sick and it doesn’t tell you that the thing you ended up with really was going to hurt you, or anything like that.”
Unfortunately, Mullis won’t be able to alert us of misinterpretation of PCR results any longer, as he passed away on August 7th 2019, shortly before this global crisis started. He has however, cautioned us about being too trusting of certain people that work within the medical field.
In this next clip, Mullis criticises Dr. Anthony Fauci, who has been the Director of the National Institute of Allergy and Infectious Diseases (NIAID) since 1984. Fauci has been one of the key members at the helm of the White House Coronavirus Task Force, after Republican senators told Donald Trump to get Fauci “more involved as the face of the federal response to the coronavirus, according to lawmakers who attended a closed-door lunch with the president.”
Kary Mullis: “Guys like Fauci get up there and start talking, he doesn’t know anything about anything. […] He doesn’t understand medicine and he should not be in the position that he’s in. […] Those guys have got an agenda, which is not what we would like them to have; being that we pay for them to take care of our health in some way. […] They make up their own rules as they go, they change them when they want to, […] Tony Fauci does not mind going on television in front of the people that pay his salary and lie directly into the camera.”
Over the past year, a myriad of doctors and scientists have voiced their concerns about using Mullis’ PCR method as a diagnostic tool, because of its high sensitivity and general unreliability. On August 29th 2020, The New York Times published an analysis on false positives given by PCR results, concluding that “In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus.” Meaning that those 90% of people are most likely not a risk of infection to others. “Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no particular risk – akin to finding a hair in a room long after a person has left,” says Dr. Michael Mina, an epidemiologist at the Harvard T.H. Chan School of Public Health.
Back in 2007, The New York Times published an article with the headline, Faith in Quick Test Leads to Epidemic That Wasn’t. Which is about using PCR to test for whooping cough at Dartmouth-Hitchcock Medical Center. “Pseudo-epidemics happen all the time. The Dartmouth case may have been one of the largest, but it was by no means an exception, […] their very sensitivity makes false positives likely, and when hundreds or thousands of people are tested, as occurred at Dartmouth, false positives can make it seem like there is an epidemic.”
Another important peer reviewed report published by 22 independent researchers, reveals ten major scientific flaws in using RT-PCR to detect SARS-CoV-2. “If someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97%.”
The most crucially important thing to remember about the PCR method, is that it isn’t testing for a virus, because fundamentally, it isn’t a test at all. It simply identifies and amplifies a specific genome sequence, for which other types of genetic material, including exosomes which naturally occur in the human body, could give a positive result for as well.
Spanish virologists found traces of the genome sequence for SARS-CoV-2 in Barcelona waste water after testing sewage water samples from March 2019, nine months before the novel coronavirus was said to be identified in China. “The levels of SARS-CoV-2 were low but were positive,” stated research leader, Albert Bosch.
Another, rather unusual, news story came out of Tanzania. After their president, John Magufuli, dismissed imported testing kits after samples taken from a goat, a sheep, a kware bird, and a papaya fruit tested positive after being sent back to the national lab assigned with human names and ages.
A similar trial was done by Italian scientists who used a different type of test, a lateral flow test, which is used as a rapid test to detect SARS-CoV-2. They used a lateral flow test to see if a kiwi would test positive for Covid-19; which it did.
Yet another widely used method of detecting SARS-CoV-2 in people is using a serology, or antibody test. Although according to the CDC, “there is a chance a positive result means that you have antibodies from an infection with a virus from the same family of viruses (called coronaviruses), such as the one that causes the common cold.” However, this statement has since been deleted from their website, but can still be found through web.archive.org.
Besides all the problems that using PCR in this manner brings along with it, matters have been made worse by counting thousands upon thousands of people who didn’t die of the novelcoronavirus, but with the novel coronavirus as covid deaths in many countries. Often while having tested positive after their deaths. Even for those who died of suicides, traffic accidents, and gunshot wounds.And besides all of the problems with people who died of clear alternate causes being counted as covid deaths, tens of thousands of test results have been double counted. And to top that off, thousands of people that had never even been tested, or people that had tested positive but died months later of alternate causes have also been added to the deaths tolls in multiple countries.
The reason I mention using PCR as a diagnostic tool, and the problems with its high sensitivity and likeliness to give false positives, at the very beginning of this article; is because all other measures are fundamentally built upon this flawed “test” and its, often misinterpreted, results.
Understanding this, we can clearly see that it makes no sense to keep using the amount of “cases,” which are really just positive PCR results, often from people who aren’t showing any, or only mild symptoms, as the measure for what amount of restrictions should be imposed.
Which brings us to our next topic.
Harm, Loss, and Damage caused by Lockdowns, and Additional Deaths
For months now it has been quite clear that lockdowns have been completely ineffective in combatting the novel coronavirus. In fact, most places that had the most stringent lockdowns early on have done far worse than places that had less strict, or no lockdowns at all.
So where did the idea of locking down society in 2020 come from in the first place? After people were having their doors welded shut in Wuhan in February, and the first European lockdown started in Italy on March 9th. Professor Neil Ferguson of Imperial College London, aptly nicknamed Professor Lockdown, published a computer model-based analysis on March 16th, which had not been peer reviewed. The analysis stated that if no action is taken “we would predict approximately 510,000 deaths in GB and 2.2 million in the US,” to say that these predictions were overestimated would be an understatement. Fergusson has made similar model-based predictions in the past which were also grossly overestimated. For example, the 2005 bird flu, for which he estimated up to 200 million deaths, while only 282 occurred between 2003 and 2009 worldwide. Three days after Ferguson published the analysis the U.K. government stated “As of 19 March 2020, COVID-19 is no longer considered to be a high consequence infectious disease (HCID) in the UK.” Four days after that, the first U.K. lockdown started on March 23rd. And two days after that, Ferguson drastically downgraded his estimates, stating that “UK deaths are now unlikely to exceed 20,000, and could be much lower.” Crediting the lockdown for the sudden drop in estimated deaths. And finally, less than a month and a half after that, Ferguson resigned in disgrace after breaking his own lockdown restrictions by inviting his married lover over to his house.
Ferguson’s analysis is what convinced Boris Johnson, the U.K. Prime Minister, to start the lockdowns and other measures. Shortly after, the rest of the world followed their example.
The detrimental effects that locking down entire countries has had, and is still having, are causing problems much worse than the virus could have ever caused, especially in poorer countries. Here are just a few examples of the damage lockdowns have caused, so far.
Every two years, the World Bank publishes an estimate of global extreme poverty, which they define as living on less than $1.90 a day, or about $700 a year. In 2020, global extreme poverty was expected to be on the rise for the first time in 20 years. “The COVID-19 pandemic is estimated to push an additional 88 million to 115 million people into extreme poverty this year, with the total rising to as many as 150 million by 2021.”
The Lancet Global Health Journal published an article stating that according to the World Food Programme “the number of people facing acute food insecurity stands to rise to 265 million in 2020, up by 130 million from the 135 million in 2019, as a result of the economic impact of Covid-19.”
Five U.N. agencies published their annual report titled, The State of Food Security and Nutrition in the World, in which they estimate just about the same as the World Food Programme did. “Preliminary projections based on the latest available global economic outlooks, also presented in this report, suggest that the COVID-19 pandemic may add an additional 83 to 132 million people to the ranks of the undernourished in 2020.”
UNICEF estimates that “an additional 6,000 children could die every day from preventable causes over the next six months as the COVID-19 pandemic continues to weaken health systems and disrupt routine services,” based on an analysis from Johns Hopkins Bloomberg School of Public Health, published in The Lancet. “Based on the worst of three scenarios in 118 low-and middle-income countries, the analysis estimates that an additional 1.2 million under-five deaths could occur in just six months,”
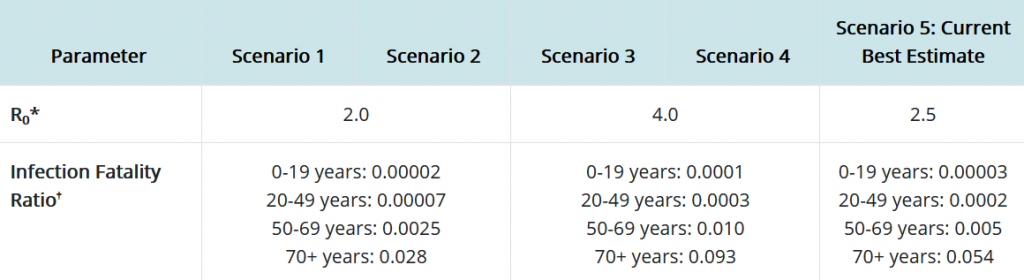
All of this, as a direct result of the lockdowns. In the name of protecting the 0.054% above 70 years of age who are at risk of dying of Covid-19, according to the CDC’s current best estimates. Does this really seem fair, or even logical in any way? To me, it certainly doesn’t.
It makes more sense to focus on protecting the relatively tiny group of people that are actually vulnerable and might actually become ill or die of the new coronavirus. This strategy, called focused protection, has been suggested by Dr. Martin Kulldorff, professor of medicine at Harvard University, Dr. Sunetra Gupta, immunology expert at Oxford University, and Dr. Jay Bhattacharya, professor at Stanford Medical School. Together they’ve written the Great Barrington Declaration, in which they argue that “Those who are not vulnerable should immediately be allowed to resume life as normal.” This is based on the premise that reaching herd immunity would be the most efficient and effective way to further combat the risk of infection for all. “As immunity builds in the population, the risk of infection to all – including the vulnerable – falls.” The Great Barrington Declaration has been translated into 43 different languages and been signed by over 57,000 medical practitioners and public health scientists, and by over 790,000 concerned citizens. The declaration can be read and signed at gbdeclaration.org.
Besides the hundreds of millions of estimated additional deaths in poorer countries, the Western World is also being directly affected by lockdowns and business closures. While these numbers don’t weigh up against the ones I just mentioned, they are still of high importance.
In an open letter written to former U.S. President Donald Trump, over 600 physicians voiced their concerns about the adverse effects that lockdowns are having, calling lockdowns a “mass casualty incident” in medical terms. Mentioning that in the U.S. suicide hotline calls have increased by 600%, 150,000 people per month that would have had new cancer detected through routine screening, an increase in child abuse, and preventable cases of strokes and heart attacks. As well as liquor sales increasing between 300-600%, cigarette sales having increased, people not being able to pay their rent, family relationships becoming frayed, and many more horrible consequences directly linked to locking down society.
A systematic review and meta-analysis has been conducted regarding the psychological impact of the novel coronavirus among healthcare workers, the general population, and patients with higher Covid-19 risk. Using data from Embase, PubMed, Google Scholar and the WHO Covid-19 databases; looking at 9207 studies, of which 62 of those studies had 162,639 participants from 17 countries. Concluding that “the COVID-19 pandemic has caused heavy psychological impact among medical workers and the general public. Psychological interventions identifying and targeting people with heavy psychological burdens are in urgent need.”
The Well Being Trust in Oakland, California, published an analysis seeking to determine how many deaths of despair, meaning deaths from drug/alcohol abuse or suicide, will occur in the US as a result of the coronavirus crisis. “Across nine different scenarios, the additional deaths of despair range from 27,644 to 154,037, with 75,000 being the most likely.” It is important to note that these figures are additional deaths, so these numbers are added to the already existing amount of deaths of despair in the United States.
In Japan, more people have committed suicide last October than have died of Covid-19 in the previous 10 months of 2020. “The monthly number of Japanese suicides rose to 2,153 in October, according to Japan’s National Police Agency. As of Friday, Japan’s total Covid-19 toll was 2,087,” Michiko Ueda, an associate professor at Waseda University in Tokyo, and an expert on suicides stated “We didn’t even have a lockdown, and the impact of Covid is very minimal compared to other countries, but still we see this big increase in the number of suicides. That suggests other countries might see a similar or even bigger increase in the number of suicides in the future.” Japan is one of the few countries to disclose timely suicide data. The most recent national data from the U.S., for example, is from 2018.
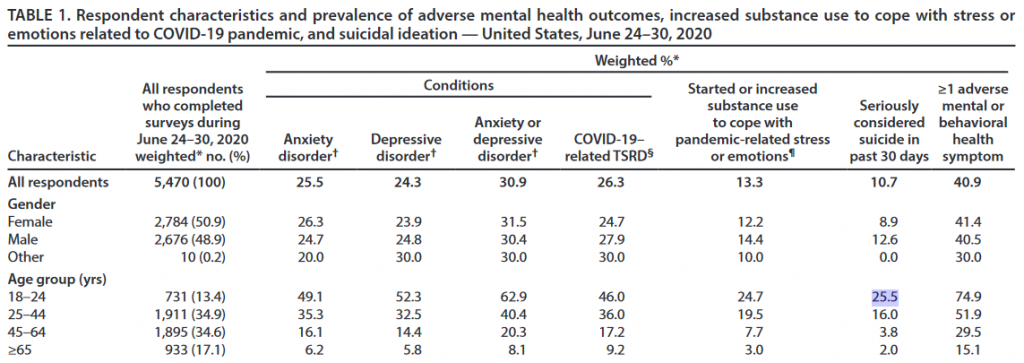
Some data we do have regarding suicide in the U.S. from 2020, comes from a report published by the CDC last August. The report states that in the age group of 18-24 year olds “25.5% seriously considered suicide in the past 30 days.”
Besides all the deaths directly linked to lockdowns, there have also been a lot of additional deaths that have been due to cancelled operations, undiagnosed cancers and other diseases, and people being afraid of going to the hospital with fear of themselves catching, or infecting someone else with the novel coronavirus.
The British Journal of Surgery published a modelling study estimating that coronavirus disruption will lead to over 28,4 million operations being cancelled or postponed worldwide during the peak twelve weeks of disruption. “Each additional week of disruption to hospital services will be associated with a further 2.4 million cancellations.”
The Social Science Research Network and The Lancet published a study on excess deaths among older adults without confirmed Covid-19 during lockdown. They concluded that “During lockdown people with dementia or severe mental illness had a higher risk of excess death. […] dementia patients suffered an additional 53% risk of death, and patients with severe mental illness suffered an additional 123% risk of death.”
A study funded by The Institute of Cancer Research, estimated that over the course of one year, a three month delay in surgery is likely to cause 4,755 excess cancer deaths, and a six month delay is estimated to cause 10,760 excess cancer deaths in the United Kingdom.
Matt Hancock, the U.K.’s Health Secretary, warned that cancer patients will only be guaranteed treatment if Covid-19 stays ‘under control.’ “Almost 2.5 million people missed out on cancer screening, referrals or treatment at the height of lockdown, even though the NHS was never overwhelmed – despite fears it would be crippled by the pandemic. Experts now fear the number of people dying as a result of delays triggered by the treatment of coronavirus patients could even end up being responsible for as many deaths as the pandemic itself.”
And as if all that wasn’t already bad enough, elderly people in the U.K. have felt “pressurised into signing Do Not Attempt CPR Forms” over the past year. Which gives doctors permission to avoid using CPR to attempt to restart a patient’s heart when it stops beating.
And besides all the deaths indirectly caused by lockdowns, a lot of people lost their livelihood, had to accept pay cuts, or even close their businesses entirely; more often than not having to close permanently. In a Local Economic Impact Report published by Yelp, they state “As of August 31, 163,735 total U.S. businesses on Yelp have closed since the beginning of the pandemic (observed as March 1), a 23% increase since July 10. In the wake of COVID-19 cases increasing and local restrictions continuing to change in many states we’re seeing both permanent and temporary closures rise across the nation, with 60% of those closed businesses not reopening (97,966 permanently closed).” And these are only the businesses that are registered on Yelp, which suggests the actual amount is much higher.
Despite all this data, governments across the world still continue to use lockdowns even after David Nabarro, special envoy on Covid-19 for the WHO stated they do not advocate lockdowns as the primary means to control the virus.
However, there’s a relatively small amount of people that the coronavirus crisis has been exceptionally good to. Namely, the world’s billionaires. As their accumulated wealth has soared to a record high of $10.2 trillion. All while the rest of the world is becoming poorer and poorer. Frequently updated reports about this can be found at inequality.org.
So, if lockdowns are causing such immense damage and harm worldwide, why are they even continuing at all? The answer is really quite simple, it’s because the only thing governments seem to be looking at are the amount of positive PCR results; those “tests” which aren’t tests, of which the inventor said it shouldn’t be used to diagnose disease.
One more peculiar thing that happened over 2020, is that the flu seems to have completely vanished off the face of the Earth. As can be seen in this graph taken from the WHO’s FluNet Charts, there are flu cases each year for the entire year. Except in 2020, where they just disappear almost entirely after week 18. Now of course, the flu hasn’t gone anywhere, and people are still catching the flu all over the world. However, because it is said that Covid-19 causes flu like symptoms, it became rather difficult to tell the difference between the two. Meaning that many people who got sick with, and/or died of the flu in 2020, were highly likely designated as covid deaths or cases.
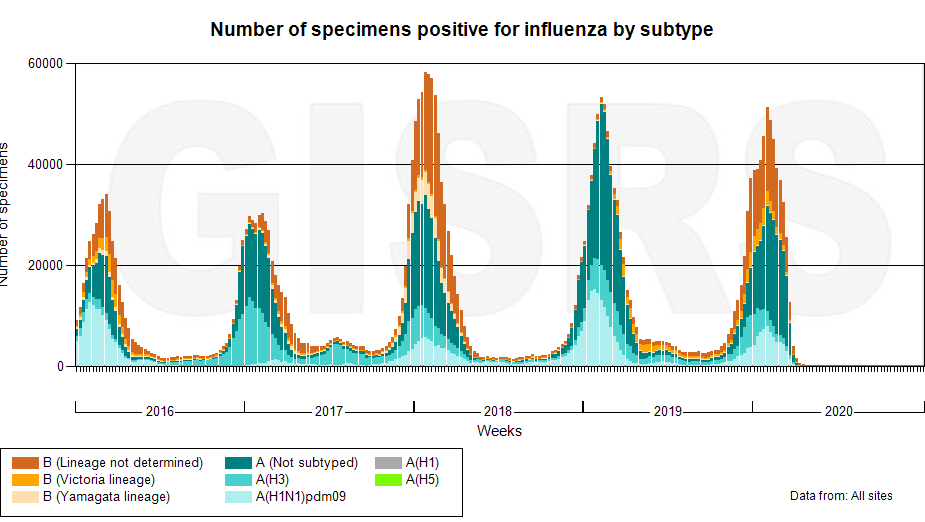
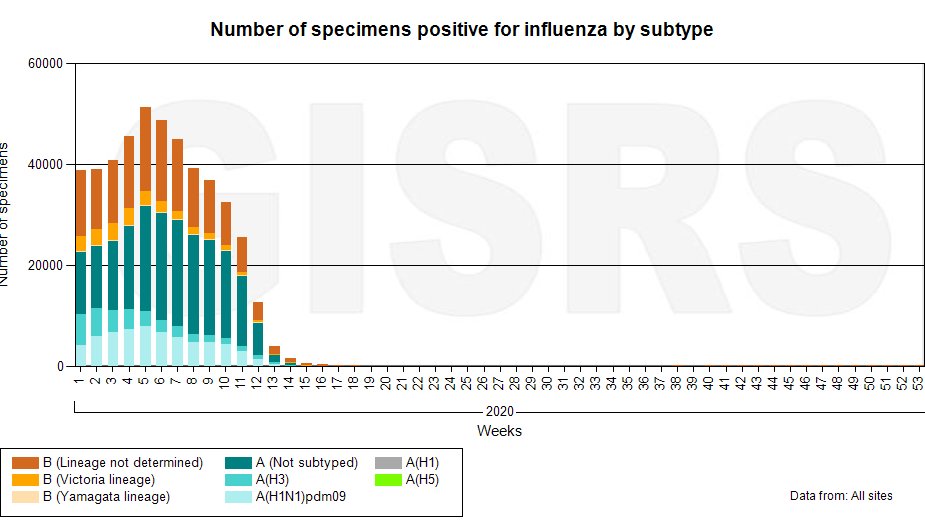
Another interesting thing to note about these charts is the high amount of positive flu cases between 2017 and 2018. During that flu season 810,000 people were hospitalised in the U.S., while by November 15th 2020 there had been a cumulative amount of 516,820 people hospitalised for Covid-19 after a positive PCR result. Meaning that by November, the amount of people hospitalised in the U.S. for Covid-19 was at 63.8% of the 2017/2018 flu season. I don’t remember there being any talk of lockdowns, physical distancing, or wearing face masks at the time. Conveniently enough, shortly after that, the CDC stopped keeping track of the cumulative amount of people hospitalised for Covid-19 altogether, because these cases are now all being classified under the same category, as PIC cases, which stands for pneumonia, influenza, and covid. Before that time, these were classified as either CLI, or ILI cases, which stands for covid-like illness and influenza-like illness, respectively.
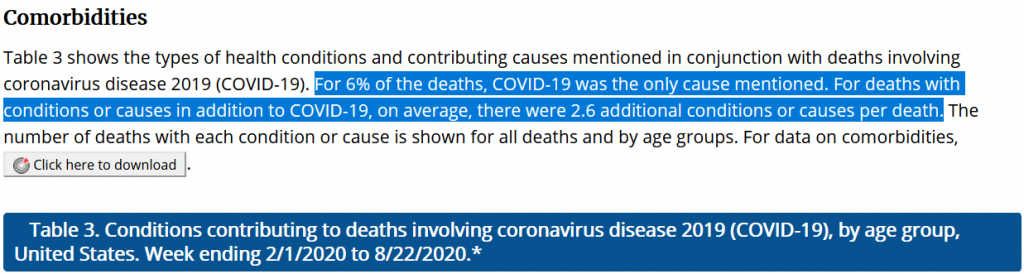
Yet another thing to note about all this, is that last August the CDC published an update regarding covid deaths, stating that only 6% of all deaths in the U.S. “involving Covid-19,” had covid mentioned as the only cause of death. This means that 6% of all 161,392 deaths were solely from covid; that’s 9,683 deaths. The other 94% had 2.6 (now updated to 2.9) additional conditions or causes contributing to their deaths, and most of those people were between 74-85 years of age or older. Meaning that almost all people that died of Covid-19 in the U.S. were people that were around 80 years old, with at least one underlying cause contributing to their death, but more than one underlying cause in nearly all cases.
In light of everything I’ve just mentioned, I’m finding it very hard to understand why anyone would still think it’s a good idea to lock down society, besides perhaps when relying and focusing exclusively on positive PCR results and ignoring all the damage and death that lockdowns are still causing. There doesn’t seem to be any logical basis for it. Nor is there any for adding clear non-covid deaths to the coronavirus death toll, or for designating people that were never even tested as covid deaths. And all the cancelled surgeries explain any excess deaths that have been occurring, and will continue to occur for the foreseeable future, if we continue on this same downhill slope.
Which brings us to the next topic to cover.
Surveillance Expansion and Government Overreach
The idea of using a pandemic to expand global surveillance and control instruments is not new. As early as 2010, the American Rockefeller Foundation described, what they call, a ‘Lock Step’ scenario in a report on future technological and international development, in which current developments are anticipated with impressive accuracy. They describe “A world of tighter top-down government control and more authoritarian leadership, with limited innovation and growing citizen pushback.”
Multiple studies have been published which predicted governments become authoritarian as the result of pandemics. A study from 2013 titled ‘Pathogens and Politics: Further Evidence that Parasite Prevalence Predicts Authoritarianism’ goes deeper into a “parasite stress hypothesis,” which proposes that when a species faces parasites and diseases their values are shaped by the experience. In this context, “parasite” is used to refer to any pathogenic organism, including bacteria and viruses. The study explains how humans react to perceived threats and how that relates to the type of government people will put up with and accept. “According to a “parasite stress” hypothesis, authoritarian governments are more likely to emerge in regions characterized by a high prevalence of disease-causing pathogens. […] At a psychological level of analysis, empirical evidence reveals that the subjective perception of infection risk causes individuals to be more conformist, to prefer conformity and obedience in others, and to respond more negatively toward others who fail to conform.” The researchers concluded that “while other threats can also influence individuals’ conformist and ethnocentric attitudes, the perceived threat of infectious disease has effects that are empirically unique,”
Similar conclusions were drawn in a study from 2011 titled ‘Threat(s) and Conformity Deconstructed: Perceived Threat of Infectious Disease and its Implications for Conformist Attitudes and Behavior.’ The most disturbing part of this particular study is that an individual’s perception of vulnerability to infection does not necessarily need to be accurate or even real to produce a profound psychological effect. If an individual perceives they are vulnerable to infection they tend to prefer conformity and accept authoritarian measures, even if they are not actually under threat of infection. “Our experimental manipulation focused on perception, not reality,” the researchers note.
These studies clearly show a link between authoritarian governance and conformist mind-sets in response to a perceived threat of infection from a disease. If we look at what is taking place around the world today regarding the coronavirus, their hypothesis is being proven correct.
A few of the authoritarian measures that have been implemented in multiple countries are: lockdowns, curfews, tracking movements, contact tracing, quarantine and isolation, temperature checks, drone surveillance, trying to mandate vaccination or making life difficult for those who refuse, police checkpoints and expanded surveillance, immunity passports and freedom passes, retention of DNA profiles, facial recognition technology, and forced quarantine facilities.
New Zealand is one of the countries that has been imposing compulsory isolation on its citizens and visitors in these quarantine facilities, for a minimum of 14 days. Since last April, when only one person had died of covid in New Zealand, the “managed isolation” is mandatory for every person arriving into New Zealand. And since August all confirmed “cases” (i.e. positive PCR results) are to go into forced isolation as well. Now to clarify, these aren’t literal prison camps or anything like that, most of the facilities are within regular hotels. However, they are being guarded by the police, AvSec (NZ Aviation Security), and the military. Multiple people, including an entire family of five, have tried to escape the forced quarantine, but all were caught shortly after and charged to different degrees.
And as icing on the cake, anybody returning to New Zealand for less than 90 days; or returning after the added regulations came into effect August 11th, will have to pay $3,100 NZ (roughly $2,230 US) for their 14 day compulsory quarantine.
In this next clip (7:40), Jacinda Ardern, Prime Minister of New Zealand, explains that people can no longer refuse to be tested or they will be held in the facilities for an additional 14 days. Remember that these are the exact same “tests” that have been proven to be flawed and inaccurate in just about every way possible.
Another person that has been at the forefront of this fiasco is Dr. Tedros Adhanom Ghebreyesus, who is not a medical doctor but happens to be the current Director-General of the WHO. In this clip Tedros states that more testing is the only way we can ever get out of our current predicament.
Dr. Tedros has a rather unsettling past, as he has been accused of covering up three separate cholera epidemics in 2006, 2009 and 2011 while working as the Minister of Health of Ethiopia. Tedros used to be a leading member of the violent and powerful communist Ethiopian political party known as the Tigray People’s Liberation Front (TPLF), which has been listed in the Global Terrorism Database for 12 separate terrorist attacks that claimed the lives of over 300 people. Human Rights Watch and many other international organisations have widely criticized the TPLF led government for crimes against humanity and atrocities towards the Ethiopian people. The TPLF has also spent millions of dollars in financial support for Tedros’ candidacy in the WHO. And as if all that wasn’t already enough, in December 2020 an article was written stating Tedros may face genocide charges after David Steinman, an economist and campaigner nominated for the Nobel Peace Prize in 2019, stated in International Criminal Court in The Hague, the Netherlands, that Tedros “was a crucial decision maker in relation to security service actions that included killing, arbitrarily detaining and torturing Ethiopians. […] causing serious bodily and mental harm to, members of the Amhara, Konso, Oromo and Somali tribes with intent to destroy those tribes in whole or in part.”
This seems like the very last person that should be in charge on anyone’s health, let alone of the World Health Organisation. Genocide and healthcare seem to be rather far apart from one another.
The fact that people like this are in the positions they’re in and dictating the lives of billions of people worldwide is not a good sign. We can clearly see that in where we now find ourselves, and the direction we’re still heading in. Namely, more surveillance, more government control, more isolation, more loss of rights and freedom, and ultimately more loss of human life.
Asymptomatic Transmission
Another hugely important element of this crisis has been alleged asymptomatic transmission of the virus; meaning that SARS-CoV-2 is detected in someone but symptoms never develop. It quickly became the narrative that anyone who has a cough, a cold or a headache could very well be infected with the novel coronavirus. And that even if you aren’t showing any symptoms whatsoever, you could very well be infected with the novel coronavirus but be asymptomatic and still able to infect others. This is what has been, and is still being proclaimed by governments and the media worldwide over the entire course of this past year. This is also the one and only reason that healthy people have been wearing face masks, isolating themselves, and going along with all the other measures for fear of inadvertently infecting someone else.
Let’s have a look at what some of the scientific literature says about asymptomatic transmission. Starting with the largest scale study on this subject, by far.
Last November, Nature Communications published a citywide screening of SARS-CoV-2 infection in nearly 10 million residents of Wuhan, China. The researchers found that there was “no evidence of transmission from asymptomatic positive persons to traced close contacts. […] The screening of the 9,865,404 participants without a history of COVID-19 found no newly confirmed COVID-19 cases, and identified 300 asymptomatic positive cases […] Of the 300 asymptomatic positive cases, two cases came from one family and another two were from another family. There were no previously confirmed COVID-19 patients in these two families. A total of 1174 close contacts of the asymptomatic positive cases were traced, and they all tested negative for COVID-19. […] Of the 34,424 participants with a history of COVID-19, 107 tested positive again, giving a repositive rate of 0.310%.”
As early as March of 2020, an Italian immunology professor from the University of Florence concluded in a study on 3,000 people that 50-75% of people of all ages that tested positive remain completely symptom free. The professor mentions that it’s important to keep in mind that these people might still be able to spread the virus to others. But again, this was back in March when there was barely any information available regarding asymptomatic transmission.
What I want to emphasise here is that if up to 75% of people testing positive don’t develop any symptoms, and therefore wouldn’t know if they’ve ever been infected or not. Imagine how many people would have already caught the virus and recovered from it. Keeping in mind the previous study in Wuhan noted that of 34,424 participants that had previously tested positive, only 107 subsequently tested positive again, a rate of 0.31%. Back in July, a Harvard University modelling study published in Nature, concluded that up to 87% of infections went unnoticed. Another study done in Wuhan which was published way back in March estimated the infection fatality rate (IFR) between 0.04 – 0.12%. Another study indicating that 78% of new infections were asymptomatic. And a report concluding that even in 70-79 year olds, about 60% remained asymptomatic.
These findings imply that virtually everyone on the planet has already been infected and recovered at some point.
This has been further emphasised, albeit accidentally, by Dr. Michael Ryan, Head of Emergencies at the WHO. Last October he stated that the agency’s best estimates indicate that roughly 1 in 10 people worldwide may have been infected by the coronavirus, which is more than 20 times the number of confirmed cases. The global population is currently around 7.8 billion people, if 10% have been infected that would be 780 million cases. The global death toll attributed to SARS-CoV-2 at the time was 1,061,539. Which would put the infection fatality rate at roughly 0.14%, which is over 24 times lower than the WHO’s provisional figure of 3.4% back in March. The 0.14% puts it right in line with seasonal flu and aligns with the estimates of many experts from all over the world.
Back in August, Dr. Maria van Kerkhove of the WHO had already stated that based on several studies, the WHO dropped the coronavirus mortality rate to around 0.6%. Another statement made by Dr. van Kerkhove with regards to asymptomatic transmission, is that many asymptomatic cases are being identified solely through contact tracing, which is another important puzzle piece regarding this particular subject, but I will get to that slightly later. Pertaining to asymptomatic transmission she stated “It’s very rare.”
A study was done in which an “asymptomatic virus carrier” was exposed to 455 contacts, of which “all the 455 contacts were excluded from SARS-CoV-2 infection.”
Which brings me back to the point that Dr. Maria van Kerkhove made about most of these studies being based on contact tracing. As far as I’ve been able to find, just about all of these studies are based exclusively on contact tracing. Here’s yet another example of a study published in a report titled ‘Evidence Summary for Asymptomatic Transmission of Covid-19’ which concludes that “risk of transmission increases as the symptoms of the source case worsen and report that of 305 close contacts of an asymptomatic patient, only one was infected, a rate of 0.33%.” Let’s look at another, an article published by The Korea Herald claimed this study offered “evidence” of asymptomatic Covid-19 transmission. The article states “a passenger on an evacuation flight from Milan to Seoul appears to have contracted the disease after sharing the same bathroom as an asymptomatic patient.” That hardly sounds like evidence to me. Especially when reading she was on board with another 298 passengers. While also taking into account that the flight time from Milan to Seoul is at least 12 hours; had none of the other 298 passengers used that same bathroom during the entire duration of the flight?
Here’s another study from Germany, also based exclusively on contact tracing which states “The fact that asymptomatic persons are potential sources of 2019-nCoV infection may warrant a reassessment of transmission dynamics of the current outbreak.” And yet another study on “presumed asymptomatic carrier transmission” based entirely on contact tracing. The list goes on and on.
Isn’t there a more effective way to find out if asymptomatic transmission is occurring, which is not based exclusively on contact tracing? As I stated at the beginning of this article, I’m not a scientist and this might be oversimplifying the matter. But if we, for example, conduct an experiment in which we have two people of which one has repeatedly “tested” positive for SARS-CoV-2 and isn’t showing any symptoms, and another person that has repeatedly “tested” negative. If asymptomatic positive patient-A coughs or sneezes in the face of negative patient-B, and if patient-B subsequently tests positive for SARS-CoV-2, would that not be a much clearer and direct indication of asymptomatic transmission? Again, I’m no scientist, but to me that seems like a more logical approach to prove asymptomatic transmission is actually occurring.
Although I can’t say that logic or rationality have been very prevalent at all over the past year.

So where do we go from here, you might ask. What do we do with all this information? Well to be frank, I don’t have an answer for that. If anything, after looking into all these topics, I now have more questions than I have answers. And my aim certainly isn’t to tell anybody what they should be doing.
However, I think some very important conclusions can be drawn from all this. Namely that relying exclusively on the government, social media, and the media to inform you, is probably the worst idea possible regarding where you get your news, and ultimately your worldview from. That’s just one of the many things that has astounded me in 2020, the amount of people that simply just believe without question anything they hear coming from an “official source.” Without taking even one minute to look up if what they have been told is accurate and true.
If you have access to the internet, there really is no excuse for being ignorant of these extremely important topics, which are quite literally reshaping the entire world around us and the way we see society and human life in general.
We aren’t dangerous germ-infested super spreaders that should be disinfecting our hands every chance we get, wearing face masks and shutting ourselves indoors. If anything, those are the exact things that are absolutely detrimental to our health. We should be outside breathing fresh air and get some sunlight on a daily basis, not wearing face masks if not sick or caring for someone who is sick. And isolation from others has been known to be absolutely terrible for our health for a long time now.
To most people, what you just read isn’t new information at all. And yet, everyone seems to just be going along with it. From what I’m personally hearing from most people around me, is that they’re just going along to get along, to avoid confrontation or awkward discussions and disagreements. But the effects this will have on each and every single one of us will be much worse than feeling awkward because you’re sharing uncomfortable truths at the workplace, or around your family, or anywhere else. This is much bigger than us, this is about the very things that make us feel human and alive being forcibly taken away from us. We’re being treated like small children who don’t have any say in the matter whatsoever, and the longer we continue allowing this to go on, the worse it will get. I guarantee it.
We started out with ‘two weeks to flatten the curve,’ we’re now at ‘you can’t go outside your house without covering your face, and can’t go out at all after 8PM,’ and we’re rushing towards ‘you can’t get on this plane without getting an injection.’
Despite how much this seems like some dystopian sci-fi horror film, this is very real. And if it hasn’t already affected you immensely, at some point it will.
I’m not saying any of this to sound negative or to try and instil fear in anyone, quite the opposite actually. But if we don’t deal with these issues as responsible adults right now I don’t think we’ll have much left of the world we used to know.
There are many more topics I wanted to cover in this article which I wasn’t able to get to, but which are equally as important. I will write a follow-up article to this one which will cover the topics of covid vaccines and the wearing of face masks, among other things.
Again, I want to emphasise that I’m not telling anyone what they should be doing with their lives. But the choice is up to each and every one of us personally to inform ourselves about what’s going on in the world around us. Please take the time to inform yourself. I’m afraid the future of humanity quite literally depends on it.
Thank you for having taken the time to read this article. Please feel free to share this information.





